Introduction
The intent of this website is to provide guidance and a rational of rehabilitation protocols for patients suffering from a herniated disc, specifically occurring in the lumbar spine at L4-L5. This is the most common place for a herniation to occur because of the amount of weight the lumbar segments carry and due to their range of motion. Its conventional nature necessitates the availability of accessible information.
Pathology
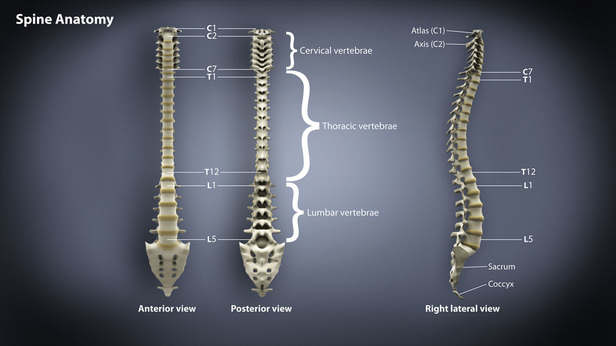
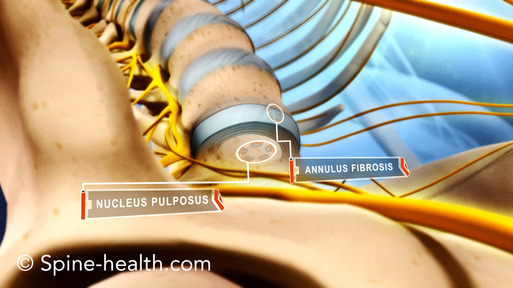
The spinal column is divided into three main sections - the cervical, thoracic, and lumbar vertebra, along with the sacrum and coccyx. Since the lumbar is at the base of the spinal column, it bears the most weight and range of motion. This excessive stress makes it the most likely place for a disc herniation to occur, especially at L4-L5. Between each vertebra is a spinal disc that consists of two main parts: the jelly-like nucleus pulpous in the disc's center, along with the outer-most layers, called the annulus fibrosis. Together they provide cushioning between the vertebra and serve as "shock absorption," along with helping to facilitate movement.
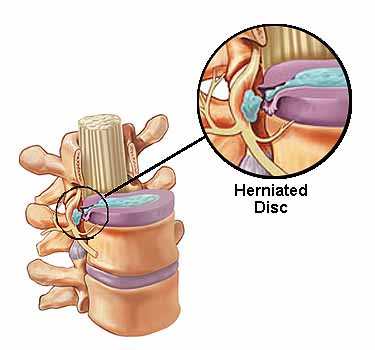
Trauma or disc degeneration can cause the nucleus to herniate through weak layers of the outer disc that causes it to leak out of the annulus fibrosus, into the spinal canal. This "weak spot" is typically underneath the spinal nerve root in the lumbar spine, meaning a herniation puts direct pressure on the nerve.


Disc degeneration occurs at different levels and stages depending upon the amount of trauma or amount of repeated stress with time. Stage I of degeneration and stage II of prolapse are considered incomplete herniations. Stages III and IV, the extrusion and sequestrian, are considered complete herniations as the nucleus pulposus is protruded through the outer layer of the disc completely, spilling out.
Etiology
Rarely does a disc herniation result from abrupt trauma such as a car accident. It is more likely from a low energy injury that progresses with time. Since there is no bloody supply to the disc, it cannot repair itself like other tissues. With aging, the nucleus pulposus loses some of its fluid properties. The thick gel in the nucleus pulposus may be forced through cracks or tears that develop in the outer layers of the disc with degeneration and age. This causes the disc to bulge, break open or herniate.
Other mechanisms that may contribute:
Risk Factors:
Other mechanisms that may contribute:
- Increased pressure to the lower back
- Mechanical, axial compression load
- Sudden, heavy strain
- Sudden twisting movement may force material out
- Repetitive stress
- Poor lifting habits
- Prolonged exposure to vibration
- Sports-related injuries
Risk Factors:
- Gender: men between 30 and 50 years of age
- Improper lifting
- Obesity/overweight patients
- Frequent driving
- Sedentary lifestyle
- Smoking
Symptomology
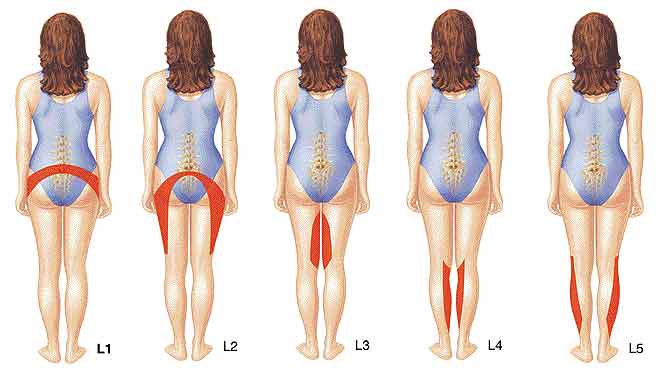
- Leg pain - sciatica, may occur with or without lower back pain
- Numbness, tingling, and/or weakness in the leg
- Lower back pain
- Butt/Glut. pain
- Loss of bladder or bowel control (rare, indicative of cauda equina syndrome)
- If nerve is impinged, there can be weakness in extending the toe, and potentially the ankle.
- Numbness and pain can be felt on top of the foot, and may radiate to the butt.
Biomechanics
- Foot drop - result of weakness from nerve impingement
- Slowed movements
- Difficulty sitting for prolonged periods
- Flexion causes most difficulty
- Exaggerated extension
